Introduction
The Pitt — Episode 3, Hank's intubation scene:
"120 of sux, 100 of ketamine." — Dr. Robby
"Good view of the glottis. Eyes off the screen. Look down the mouth and insert the tube around the bend." — Supervisor
"Now look back at the screen. Advance through the cords. Good job." — Supervisor
In under 60 seconds, Hank — the construction worker with a nail in his heart — was sedated, paralyzed, and intubated. The medication sequence administered and the video laryngoscopy technique described step by step by the supervisor portray with clinical precision what Rapid Sequence Intubation (RSI) is: the standard protocol for airway management in emergencies.
RSI is one of the most taught, most trained, and most critical procedures in all of emergency medicine. Mastering it is an indispensable requirement for any physician working in an emergency department, ICU, or advanced prehospital care.
What is Rapid Sequence Intubation?
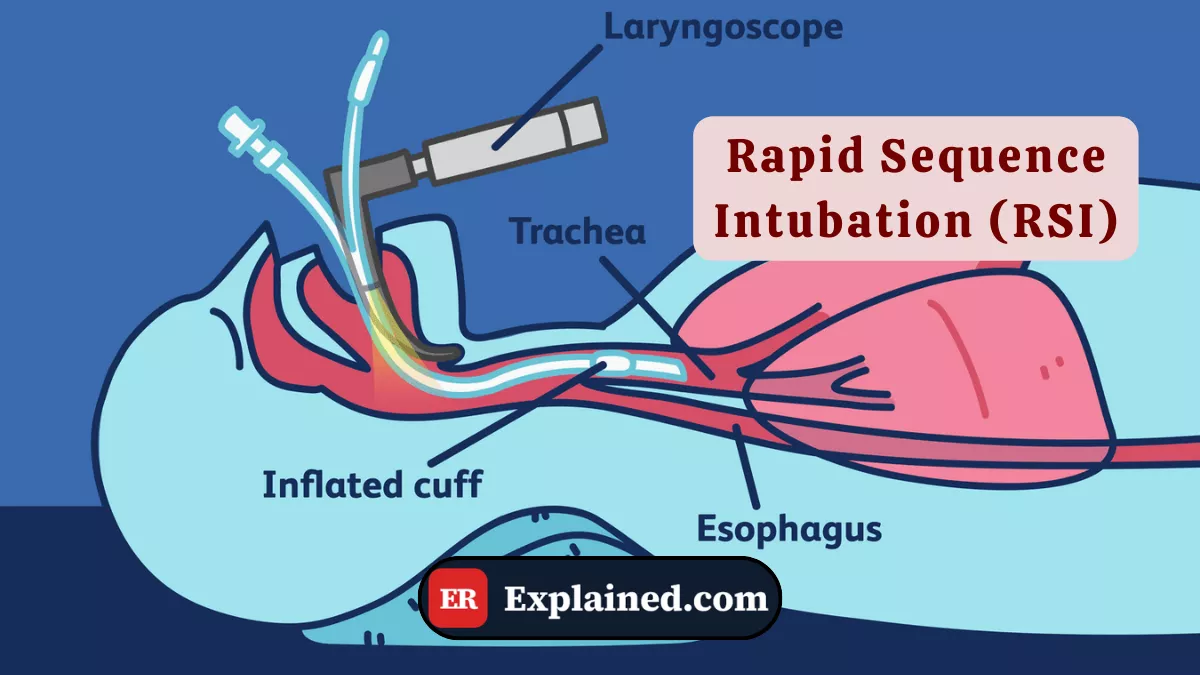
Rapid Sequence Intubation (RSI) is a standardized airway management protocol that combines the simultaneous administration of an anesthetic induction agent and an ultra-rapid-acting neuromuscular blocker to facilitate laryngoscopy and endotracheal tube passage under ideal conditions, minimizing the risk of pulmonary aspiration.

The logic of the protocol is to create a safe apnea window — a period in which the patient is sedated, with fully relaxed muscles and no airway protective reflexes, allowing direct visualization of the vocal cords and safe tube passage.
The fundamental difference between RSI and conventional intubation is speed and sequence: the two medications are administered in rapid succession, the tube is inserted as soon as effects take hold — typically in 45 to 60 seconds — and the patient is not ventilated with a mask between induction and intubation, except in cases of critical desaturation.
Causes and Clinical Context
RSI is indicated whenever a patient needs urgent intubation and presents a risk of gastric content aspiration — which includes virtually every emergency intubation. Main indications include:
- Acute respiratory failure refractory to non-invasive support
- Depressed level of consciousness — Glasgow score of 8 or below — with inability to protect the airway
- Before emergency surgical procedures — as with Hank, intubated before the thoracotomy
- Cardiac arrest requiring a definitive airway
- Extreme psychomotor agitation preventing safe management without sedation and paralysis
- Severe traumatic brain injury with risk of cerebral herniation
In the episode, the decision to use ketamine as the induction agent was deliberate: ketamine maintains blood pressure and sympathetic drive — a critical advantage in a patient with cardiac tamponade and a falling pressure. Succinylcholine was chosen for its speed of onset and short-duration neuromuscular blockade profile.
Signs and Symptoms
Situations indicating RSI have recognizable presentations. Warning signs include:
Imminent ventilatory failure:
- Respiratory rate above 35 or below 8 breaths/min
- Intense use of accessory muscles — sternocleidomastoid, intercostals, abdomen
- SpO2 below 90% despite supplemental oxygen
- Central cyanosis
Airway protection failure:
- Glasgow score of 8 or below
- Absent cough and gag reflexes
- Active regurgitation or high aspiration risk
- Inspiratory stridor — indicating partial laryngeal obstruction
Diagnosis
The indication for RSI is clinical. The main assessed parameters include:
Glasgow Coma Scale (GCS): a score of 8 or below is a mandatory indication for intubation to protect the airway.
Arterial blood gas: PaO2 below 60 mmHg with FiO2 of 0.5 or above, or PaCO2 above 50 mmHg with pH below 7.25 are gasometric intubation criteria.
Difficult airway assessment: before any RSI, the physician must evaluate difficult airway predictors — mouth opening, cervical mobility, thyromental distance, Mallampati class, and presence of beard, obesity, or facial trauma. A predictably difficult airway requires alternative planning before paralysis.
Continuous pulse oximetry: guides the urgency of intervention and monitors saturation throughout the procedure.
The RSI Protocol — The 7 Ps
The RSI protocol is classically structured in 7 sequential steps:
- Preparation: check and organize all equipment — correctly sized ETT with tested cuff, functioning laryngoscope or video laryngoscope, suction on and positioned, BVM connected to oxygen, medications in labeled syringes, capnograph ready.
- Preoxygenation: administer 100% oxygen via mask for 3 to 5 minutes. The goal is to denitrogenate the lungs and create an O2 reserve that extends the safe apnea window — up to 8 minutes in healthy patients.
- Pretreatment: specific medications based on the clinical picture. Lidocaine 1.5 mg/kg IV in traumatic brain injury to attenuate intracranial pressure elevation. Atropine 0.02 mg/kg in children under 1 year to prevent vagal bradycardia.
- Paralysis with Induction: administration of the induction agent immediately followed by the neuromuscular blocker. In the episode: ketamine 100 mg IV (approximately 1–2 mg/kg) + succinylcholine 120 mg IV (1.5 mg/kg). Alternative pair: propofol or etomidate + rocuronium 1.2 mg/kg.
- Positioning: head in sniffing position — moderate cervical extension with slight elevation of the occiput on a pad. In cervical trauma, maintain the spine in neutral position with manual stabilization.
- Placement of the tube: direct or video laryngoscopy. Visualize the vocal cords and advance the tube to 21–23 cm at the teeth in adults. Confirm placement by capnography and auscultation.
- Post-intubation management: inflate the cuff, secure the tube, connect to the ventilator with adequate initial settings, request confirmatory chest X-ray, and initiate continuous sedation and analgesia.
Prognosis and Complications
In the hands of a trained professional, RSI has a first-attempt success rate exceeding 85–90%. The use of video laryngoscopy pushes that rate beyond 95% in difficult airways.
Main complications include:
- Esophageal intubation: the most serious complication. Continuous CO2 waveform capnography eliminates this risk when used correctly.
- Right mainstem bronchus intubation: the tube advances beyond the carina. Detected by asymmetric auscultation.
- Post-intubation hypotension: caused by anesthetic agents and positive pressure ventilation.
- Desaturation during the attempt: each failed attempt consumes the O2 reserve created during preoxygenation.
- Airway trauma: laceration of lips, teeth, or vocal cords during laryngoscopy.
- Prolonged neuromuscular blockade: risk with high-dose rocuronium without sugammadex available for reversal.

Frequently Asked Questions
What is the difference between ketamine and propofol as RSI induction agents?
Ketamine is the preferred induction agent in hemodynamically unstable patients — like Hank in the episode — because it stimulates catecholamine release, maintaining or elevating blood pressure and heart rate. It is also a bronchodilator, advantageous in asthmatic patients. Propofol is excellent for stable patients but causes significant dose-dependent hypotension — contraindicated in shock.
Why is the patient not ventilated between induction and intubation?
Mask ventilation between induction and intubation would insufflate air into the stomach, increasing the risk of regurgitation and pulmonary aspiration — the primary complication RSI is designed to prevent. The exception is critical desaturation during the apnea window, when gentle ventilation is necessary to buy time.
What is a difficult airway and how does it change the protocol?
A difficult airway is one where vocal cord visualization or tube passage is predictably challenging due to the patient's anatomical features. When identified before RSI, the protocol changes: awake intubation with topical anesthesia and light sedation may be chosen, or supraglottic rescue devices as an immediate Plan B. One should never paralyze a patient with a difficult airway without a clear rescue plan.
What is the dose of succinylcholine in RSI?
The standard dose of succinylcholine in RSI in adults is 1.5 mg/kg IV. For an 80 kg adult, that equals 120 mg — exactly the dose used for Hank in the episode. In children, the dose is higher: 2 mg/kg IV. Onset is 45 to 60 seconds and blockade duration is 8 to 12 minutes — sufficient time for intubation and spontaneous recovery if the procedure fails.
Conclusion
Rapid Sequence Intubation is one of the most elegant procedures in emergency medicine — a precise choreography of medications, positioning, and technique that, when well executed, secures a definitive airway in under 60 seconds. Episode 3 of The Pitt faithfully depicted every step of this protocol, from the choice of ketamine to advancing the tube through the vocal cords under video laryngoscopy.
Explore more in our Medical Procedures category. Also read about the endotracheal tube, ketamine in the ER, succinylcholine, and the mechanical ventilator.
Disclaimer: This content is for educational purposes only and does not substitute professional medical evaluation, diagnosis, or treatment. In case of emergency, call 911 immediately.


