Introduction
The Pitt — Episode 3, cardiac tamponade scene:
"Small pericardial effusion, no evidence of tamponade." — Physician at ultrasound
"Not yet." — Dr. Garcia
"Effusion has grown, now with RV collapse. Pericardiocentesis?" — Team
This exchange reveals the central clinical dilemma surrounding pericardiocentesis: the moment to indicate it. Hank's pericardial effusion started small — still without tamponade — and rapidly progressed to right ventricular collapse, the ultrasound finding that defines absolute emergency. The team's question — pericardiocentesis? — was answered by clinical progression: no, in this case a thoracotomy would be necessary.
But in many other situations, pericardiocentesis is exactly the right answer. Understanding when to perform it, how to guide it safely, and what its limits are is essential for any emergency physician.
What is Pericardiocentesis?
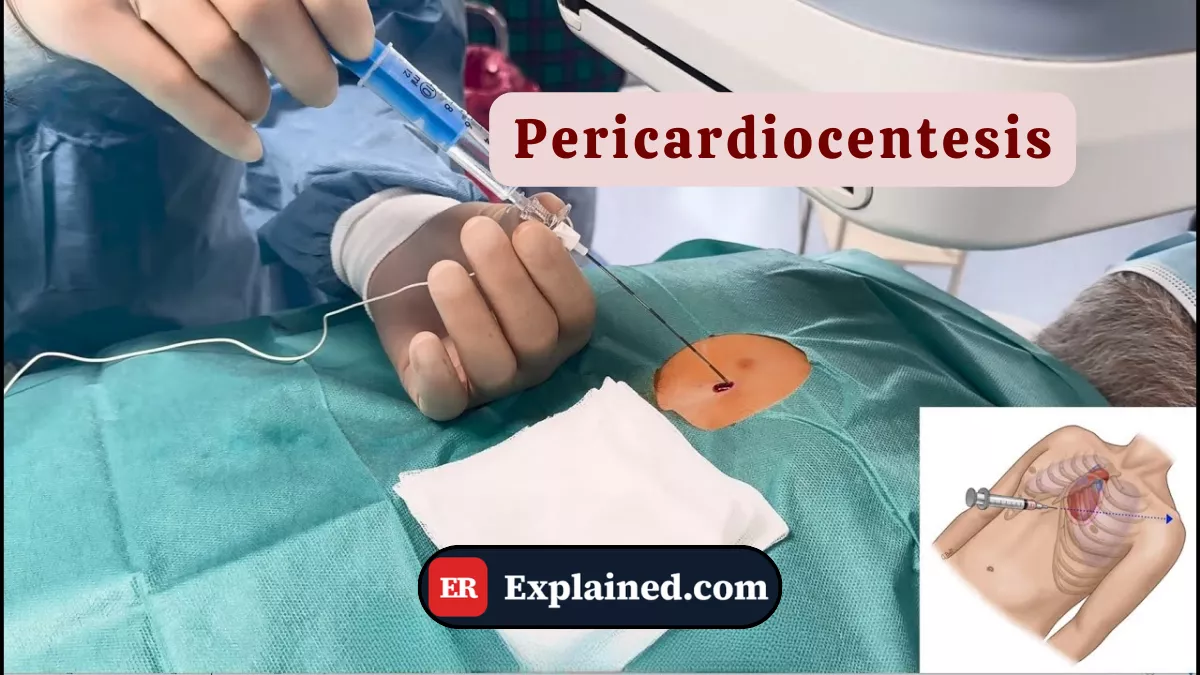
Pericardiocentesis is a minimally invasive procedure consisting of percutaneous puncture of the pericardial sac to drain fluid accumulated around the heart. When this fluid accumulates in sufficient volume and pressure to compress the cardiac chambers and impair diastolic filling, it constitutes cardiac tamponade — a potentially fatal emergency requiring immediate drainage.

The procedure can be performed in two main ways:
- Ultrasound-guided at the bedside: the preferred method today. The transducer identifies fluid accumulation in real time, guides needle trajectory, and confirms intrapericardial positioning before and during drainage.
- Blind subxiphoid approach: historical technique performed without imaging guidance, by inserting the needle below the xiphoid process toward the left shoulder. Retained in absolute emergencies without available ultrasound.
In cases of chronic or recurrent pericardial effusion, a continuous drainage catheter may be placed — the surgical pericardial window — to prevent recurrence.
Causes and Clinical Context
Causes of pericardial effusion with tamponade potential include a broad spectrum of conditions:
- Penetrating thoracic trauma: as in Hank's case, stab wounds, gunshot wounds, or penetrating objects can cause direct bleeding into the pericardial sac.
- Acute pericarditis: pericardial inflammation from viral, bacterial, autoimmune, or idiopathic causes.
- Malignancies: pericardial metastases are a frequent cause of large hemorrhagic effusions, especially in lung cancer, breast cancer, and lymphomas.
- Severe renal failure: uremia causes pericarditis and effusion through chemical inflammation of the serosa.
- Type A aortic dissection: blood from the dissection can extend into the pericardial sac.
- Post-cardiac surgery: bleeding into the pericardial space after open cardiac procedures.
- Severe hypothyroidism: causes slowly progressive pericardial effusion, usually without acute tamponade.
The rate of accumulation matters more than the absolute volume. Rapid bleeding of 200 ml can cause fatal tamponade, while a chronic 2-liter effusion may be tolerated by a pericardium that has gradually stretched over weeks.
Signs and Symptoms
Cardiac tamponade classically presents with Beck's triad:
- Hypotension — systolic pressure below 90 mmHg, refractory to fluids
- Muffled heart sounds — distant or inaudible heart sounds on auscultation
- Jugular venous distension — neck vein engorgement from elevated central venous pressure
Other important signs include:
- Pulsus paradoxus: drop in systolic pressure greater than 10 mmHg during inspiration — highly sensitive sign of tamponade
- Compensatory tachycardia
- Progressive dyspnea and orthopnea
- Anxiety, agitation, and sense of impending doom
- In severe cases: obtundation and distributive shock
On ultrasound, diastolic collapse of the right ventricle is the most specific finding of hemodynamic tamponade — exactly what the team detected in Hank's evolving presentation.
Diagnosis
The diagnosis is clinical and sonographic:
Point-of-care ultrasound (subxiphoid window): identifies the effusion as an anechoic band around the heart. Diastolic RV collapse is the sign of hemodynamic tamponade. The complete exam takes under 2 minutes.
ECG: may show diffuse low voltage and electrical alternans — cyclic variation in QRS morphology caused by the pendular movement of the heart within the pericardial fluid. It is a late and specific sign of a large effusion.
Chest X-ray: cardiomegaly with flask-shaped cardiac silhouette in large chronic effusions. Of limited use in acute emergencies.
CT scan: excellent for quantification and localization of the effusion in stable patients, but rarely available before emergency pericardiocentesis.
The Procedure in the ER
Ultrasound-guided pericardiocentesis follows this protocol:
- Position the patient supine with the head elevated 30–45° — so fluid pools in the inferior portion of the pericardial sac.
- Set up continuous monitoring: ECG, pulse oximetry, and blood pressure.
- Anesthetize the skin and subcutaneous tissue with 1% lidocaine at the puncture site.
- Cover the ultrasound transducer with a sterile sheath to guide the procedure aseptically.
- Identify the ideal access window — usually apical or subxiphoid — where the effusion is largest and the skin-to-fluid distance is smallest.
- Insert a large-bore needle (16–18G) under real-time ultrasound visualization, advancing toward the fluid.
- Confirm intrapericardial position by visualizing the needle tip within the fluid space.
- Introduce the guidewire through the needle (Seldinger technique), remove the needle, and dilate the tract.
- Insert the drainage catheter over the guidewire and connect to a closed drainage system.
- Drain fluid slowly — hemodynamic improvement typically occurs after the first 50 to 100 ml are removed.
- Collect samples for laboratory analysis: cytology, culture, LDH, proteins, and glucose.
- Secure the catheter to the skin and maintain continuous drainage based on reaccumulation rate.
In the episode, pericardiocentesis was considered but replaced by thoracotomy because the tamponade was hemorrhagic from a traumatic source — a situation where percutaneous drainage would be insufficient to control active bleeding and could delay definitive intervention.
Prognosis and Complications
When correctly indicated and performed with ultrasound guidance, pericardiocentesis has a success rate exceeding 95% and a low rate of serious complications.
Main complications include:
- Myocardial or coronary artery laceration: the most serious complication, generally caused by inadvertent puncture of the cardiac wall.
- Pneumothorax: from puncture of the adjacent pleura.
- Cardiac arrhythmias: especially when the needle contacts the epicardium.
- Pericardial infection: rare with adequate aseptic technique.
- Pneumopericardium: air entry into the pericardial space.
- Effusion reaccumulation: frequent in malignant and infectious causes without treatment of the underlying etiology.
Ultrasound guidance reduced the rate of serious complications from approximately 6% (blind technique) to less than 1.5% (guided technique).

Frequently Asked Questions
What is the difference between pericardiocentesis and surgical drainage?
Percutaneous pericardiocentesis is a minimally invasive bedside procedure using a needle and catheter guided by ultrasound. Surgical drainage — or pericardial window — is a surgical procedure that creates a permanent opening in the pericardium for continuous drainage, indicated for recurrent effusions, traumatic hemorrhagic tamponades, or when percutaneous pericardiocentesis fails or is insufficient.
Does the patient feel pain during pericardiocentesis?
With adequate local anesthesia using lidocaine, the procedure is well tolerated in conscious patients. Pressure and discomfort sensations are common during needle advancement. Very anxious patients or those in severe hemodynamic instability may receive additional light sedation. Intense pain during the procedure may indicate needle contact with the epicardium — a warning to reposition.
When is pericardiocentesis not sufficient?
In hemorrhagic tamponades of traumatic origin — as in the episode — percutaneous pericardiocentesis is rarely definitive, as it drains blood but does not control the bleeding source. In these cases, emergency thoracotomy is necessary. Pericardiocentesis may be performed as a temporary stabilization measure while preparing for surgery.
What fluid is normally in the pericardial sac?
Normally the pericardial sac contains between 15 and 50 ml of serous fluid, which acts as a lubricant between the pericardial layers during cardiac movements. Volumes above 100 ml are detectable on ultrasound as an anechoic band around the heart. Volumes above 200 ml significantly increase the risk of tamponade, especially when accumulation is rapid.
Conclusion
Pericardiocentesis is one of the highest-impact emergency procedures in terms of immediate hemodynamic reversal — capable of reversing a fatal tamponade in seconds, with minimal invasiveness when ultrasound-guided. Episode 3 of The Pitt clearly showed both its indication and its limit: when bleeding is active and traumatic, surgery is irreplaceable.
Explore more in our Medical Procedures category. Also read about cardiac tamponade, point-of-care ultrasound, emergency thoracotomy, and penetrating cardiac trauma.
Disclaimer: This content is for educational purposes only and does not substitute professional medical evaluation, diagnosis, or treatment. In case of emergency, call 911 immediately.

