Introduction
The Pitt — Episode 3, Hank's intubation scene:
"Good view of the glottis. Now eyes off the screen. Look down the mouth and insert the tube around the bend." — Supervisor
"Now look back at the screen. Advance through the cords." — Supervisor
"Good job." — Team
This scene shows Hank's intubation — the construction worker with a nail in his heart — being performed by resident Javadi under direct supervision. The step-by-step technique described captures the real procedure with precision: video laryngoscopy, vocal cord visualization, and careful passage of the endotracheal tube through the glottis.
The endotracheal tube is one of the most critical devices in emergency and critical care medicine. When correctly inserted, it secures the airway, enables mechanical ventilation, and protects the lungs from aspiration. When incorrectly inserted, it can be fatal within minutes.
What is an Endotracheal Tube?
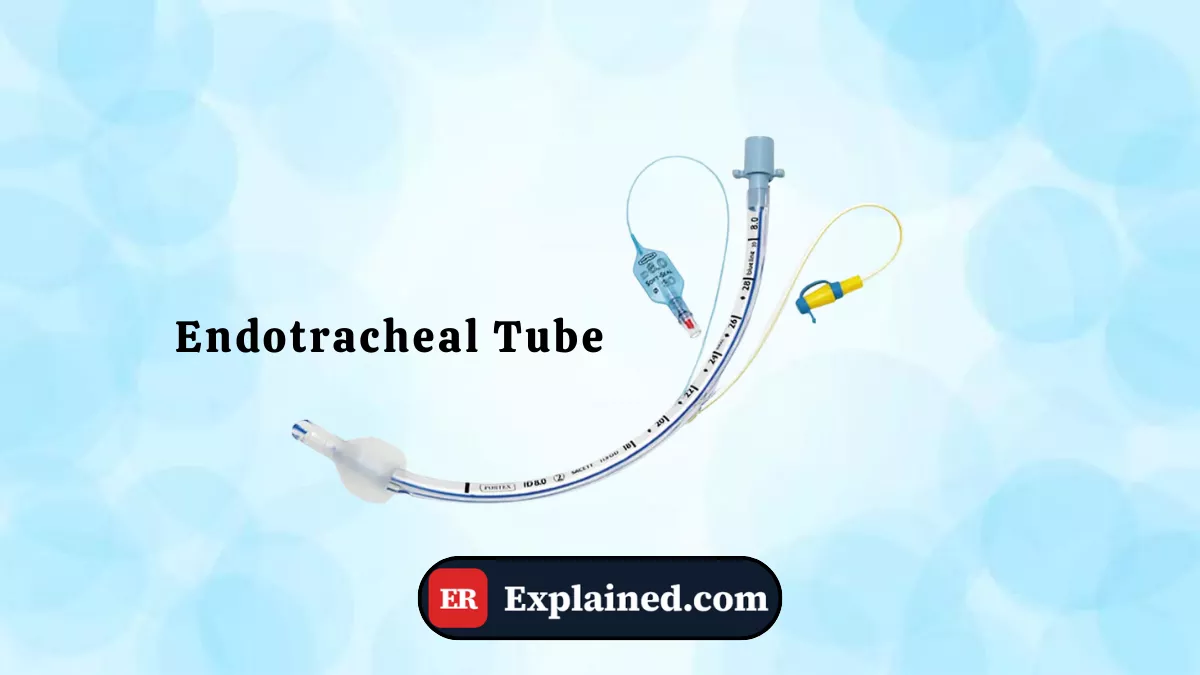
An endotracheal tube (ETT) is a flexible tubular device, typically made of transparent polyvinyl chloride (PVC), inserted through the mouth or nose into the trachea to secure a definitive and safe airway. It connects the patient to a mechanical ventilator or bag-valve-mask for manual ventilation.

Its main components include:
- Tube body: transparent cylinder with depth markings in centimeters to guide positioning.
- Cuff (balloon): inflatable balloon at the distal end that, when inflated, seals the trachea around the tube — preventing secretion entry and ensuring effective ventilation without leaks.
- Radiopaque line: wire embedded in the tube visible on chest X-ray, allowing positioning confirmation.
- 15 mm connector: universal adapter at the proximal end connecting to the ventilator or bag-valve device.
Endotracheal tubes are numbered by internal diameter in millimeters. For adults, typical sizes are:
- Men: 8.0 to 8.5 mm tubes
- Women: 7.0 to 7.5 mm tubes
- Children: calculated by the formula: (age in years ÷ 4) + 4 for uncuffed tubes
Causes and Clinical Context
Orotracheal intubation with an endotracheal tube is indicated in situations where the patient cannot maintain a patent airway or adequate ventilation independently:
- Depressed level of consciousness: Glasgow Coma Scale score of 8 or below indicates inability to protect the airway.
- Acute respiratory failure: hypoxia or hypercapnia refractory to non-invasive support.
- Cardiac arrest: early intubation secures the airway and enables effective ventilation during resuscitation.
- Before emergency surgical procedures: as in Hank's case, who needed intubation before the thoracotomy.
- Angioedema or airway obstruction: glottic edema from severe allergic reaction, trauma, or tumor.
- Aspiration protection: patients with intractable vomiting or upper gastrointestinal bleeding with depressed consciousness.
In the episode, Hank's intubation was performed using rapid sequence intubation (RSI) — the standard protocol in emergencies — using ketamine as the induction agent and succinylcholine as the neuromuscular blocker, followed by video laryngoscopy for airway visualization.
Signs and Symptoms
The situations indicating the need for intubation present recognizable clinical findings:
Signs of imminent airway failure:
- Stridor — high-pitched inspiratory sound indicating partial laryngeal or tracheal obstruction
- Inability to swallow or keep the mouth closed
- Blood, vomit, or abundant secretions in the airway
- Facial burn or smoke inhalation with risk of progressive edema
Signs of ventilatory failure:
- Extreme respiratory rate — above 35 or below 8 breaths/min
- Intense respiratory effort without clinical improvement
- SpO2 below 90% despite 15 L/min oxygen mask
- Altered level of consciousness from hypoxia or hypercapnia
Neurological signs of mandatory intubation:
- Glasgow Coma Scale score of 8 or below
- Absent cough and gag reflexes
- Prolonged seizures without recovery of consciousness
Diagnosis
The decision to intubate is clinical, but confirming correct tube positioning is fundamental and involves multiple methods:
Colorimetric or continuous capnography: the most reliable method to confirm tracheal intubation. The presence of exhaled CO2 confirms the tube is in the trachea and not the esophagus. Continuous capnography with a capnogram waveform is the gold standard.
Pulmonary and gastric auscultation: symmetric bilateral breath sounds and absence of gastric sounds suggest correct positioning — but can be misleading in obese patients or those with lung disease.
Direct visualization through the vocal cords: during laryngoscopy, watching the tube pass between the vocal cords is the most direct confirmation of correct placement.
Chest X-ray: confirms tube depth — the tip should be 2 to 3 cm above the carina, at the level of the 3rd thoracic vertebra. Mandatory after every elective intubation and whenever positioning is in doubt.
Airway ultrasound: can visualize the tube in the trachea in real time, with superior sensitivity to auscultation alone.
Emergency Use
Rapid sequence intubation (RSI) is the standard method in the emergency setting. The protocol follows the 7 Ps:
- Preparation: check equipment — correctly sized tube with cuff tested, functioning laryngoscope, suction on, bag-valve-mask connected to oxygen, medications drawn up.
- Preoxygenation: 100% oxygen mask for 3 to 5 minutes to build O2 reserve and extend the safe apnea window.
- Pretreatment: specific medications based on the clinical picture — lidocaine in head trauma, atropine in children, fentanyl in elevated intracranial pressure.
- Paralysis with induction: administration of the anesthetic induction agent followed by the neuromuscular blocker — in the episode, ketamine 100 mg + succinylcholine 120 mg IV.
- Positioning: head in sniffing position — moderate cervical extension with slight elevation of the occiput.
- Placement of the tube: direct or video laryngoscopy, vocal cord visualization, and tube advancement to 21 to 23 cm at the teeth in adults.
- Post-intubation management: inflate the cuff, confirm positioning by capnography and auscultation, secure the tube, connect to the ventilator, and request a chest X-ray.
Prognosis and Complications
Successful intubation secures the airway and ensures effective ventilation — a fundamental condition for any subsequent intervention. However, the procedure carries potential complications:
- Esophageal intubation: the most serious and preventable complication. The tube is inserted into the esophagus instead of the trachea. Fatal if not immediately recognized. Capnography eliminates this risk when used correctly.
- Right mainstem bronchus intubation: the tube advances beyond the carina into the right main bronchus, ventilating only the right lung. Detected by asymmetric auscultation and corrected by pulling the tube back.
- Airway trauma: laceration of lips, teeth, vocal cords, or trachea during laryngoscopy.
- Hypoxemia during the attempt: each intubation attempt consumes O2 and can cause desaturation — especially in patients without respiratory reserve.
- Post-intubation hypotension: anesthetic agents and positive pressure ventilation can reduce venous return and blood pressure.
- Tracheal cuff injury: excessive cuff pressure can cause ischemia and mucosal necrosis with prolonged use.

Frequently Asked Questions
Is intubation a painful procedure?
In emergency situations, intubation is performed after sedation and neuromuscular blockade — the patient does not feel pain during the procedure. In awake patients with progressive airway obstruction, it can be performed under topical anesthesia with lidocaine spray and light sedation to preserve respiratory drive — a technique called awake intubation. The main discomfort after intubation is the presence of the tube in the throat, controlled by continuous sedation while the tube is in place.
What is video laryngoscopy?
Video laryngoscopy is an intubation technique that uses a laryngoscope with a camera at the tip of the blade, transmitting the laryngeal image to a screen in real time. It significantly improves glottic visualization — especially in difficult airways — and is becoming the standard method in many emergency departments. In the episode, resident Javadi used video laryngoscopy under supervisor guidance, exactly as taught in modern clinical practice.
How long can the endotracheal tube remain in place?
There is no absolute limit, but tracheostomy evaluation is recommended after 7 to 14 days of mechanical ventilation. Tracheostomy is more comfortable, reduces laryngeal trauma, facilitates oral hygiene and ventilator weaning, and allows the patient to communicate and eat orally in some cases. The decision is individualized based on prognosis and clinical progression.
What happens when the tube is removed?
Extubation is performed when the patient recovers the ability to breathe spontaneously and protect the airway. The process includes spontaneous breathing trials, level of consciousness assessment, and evaluation of protective reflexes. Extubation may fail in up to 20% of cases — in these patients, the tube must be reinserted. In the episode, Nick Bradley's terminal extubation was a deliberate palliative act, not a conventional clinical extubation.
Conclusion
The endotracheal tube is a seemingly simple device that represents, in practice, one of the most critical and technically demanding interventions in emergency medicine. As shown in Episode 3 of The Pitt, its correct insertion requires rigorous training, adequate supervision, and precise positioning confirmation — and its removal, in certain circumstances, represents one of the heaviest decisions a medical team can face.
Explore more in our Medical Instruments category. Also read about mechanical ventilator, orotracheal intubation, ketamine in emergency sedation, and brain death.
Disclaimer: This content is for educational purposes only and does not substitute professional medical evaluation, diagnosis, or treatment. In case of emergency, call 911 immediately.


