Introduction
The Pitt — Episode 3, post-death debrief scene:
"In the hallway, he should have been on a cardiac monitor. We would have caught the arrest right away." — Resident
"True, but there was no indication for monitoring at the time." — Dr. Robby
"We now know his abdominal pain was not from gallstones but from unstable angina due to coronary artery disease." — Dr. Robby
This debrief scene following the unexpected death of Mr. Milton captures one of the most real dilemmas in emergency medicine: continuous cardiac monitoring can save lives — but it is neither feasible nor indicated to connect every patient to a monitor. The clinical decision about who to monitor, when, and for how long is one of the most critical competencies of the emergency physician.
The cardiac monitor is a constant presence in every emergency room, ICU, and observation unit. Understanding how it works, what it detects, and what its limits are is essential for healthcare professionals, patients, and families alike.
What is a Cardiac Monitor?
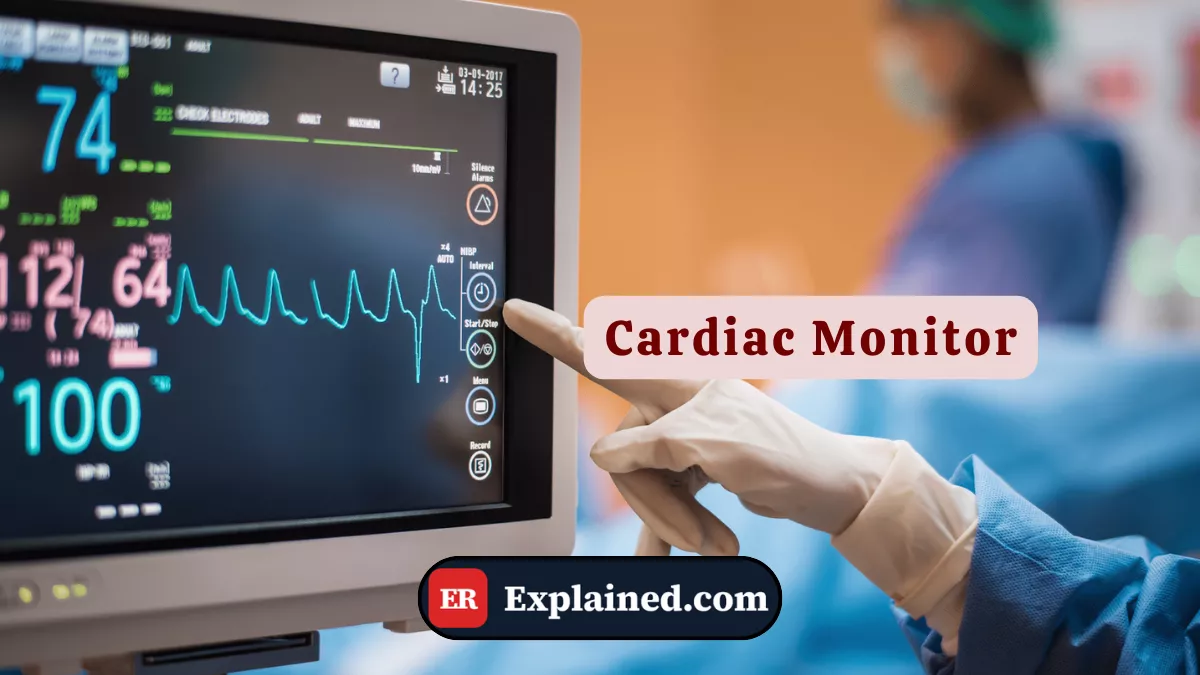
A cardiac monitor — also called a multiparameter monitor or bedside monitor — is an electronic device that continuously records and displays the patient's vital signs in real time. In the emergency setting, the monitored parameters include:

- Continuous electrocardiogram (ECG): records the heart's electrical activity, identifying rhythm, rate, and any conduction abnormalities or ischemic changes.
- Heart rate: automatically calculated from the ECG.
- Peripheral oxygen saturation (SpO2): measured by pulse oximetry, indicating blood oxygenation.
- Non-invasive blood pressure (NIBP): measured by automatic cuff at programmed intervals.
- Respiratory rate: calculated from thoracic impedance variation or flow sensors.
- Body temperature: in more complete models, via skin or rectal probe.
- Capnography (EtCO2): end-tidal CO2 measurement, essential in intubated patients.
Modern monitors are networked to the nursing station, allowing centralized supervision of multiple patients simultaneously. Audible and visual alarms alert the team to critical changes — such as falling saturation, tachycardia, bradycardia, or serious arrhythmias.
Causes and Clinical Context
The indication for continuous cardiac monitoring in the ER is based on the risk of sudden clinical deterioration. The main situations indicating monitoring include:
- Chest pain: suspected acute coronary syndrome, pulmonary embolism, or aortic dissection.
- Known or suspected arrhythmias: palpitations, syncope, presyncope, or irregular rhythm finding.
- After cardiopulmonary resuscitation: resuscitated patients have a high risk of arrhythmia recurrence.
- Intoxications and overdoses: many drugs prolong the QT interval or cause arrhythmias — such as the fentanyl and benzodiazepines seen in the episode.
- Severe electrolyte disturbances: hypokalemia, hyperkalemia, and hypomagnesemia are frequent causes of potentially fatal arrhythmias.
- Shock of any etiology: monitoring guides treatment response and detects early deterioration.
- Intubated and sedated patients: mandatory monitoring while invasive ventilatory support is in place.
In the episode, the post-death debate centered precisely on this decision: with a HEART score of 3 and initially normal tests, monitoring was not mandatory by protocol — but unstable angina silently progressed to fatal infarction before any external warning sign appeared.
Signs and Symptoms
The cardiac monitor detects changes that often precede visible clinical symptoms. The most critical monitor findings include:
Rhythm disturbances:
- Ventricular fibrillation — completely chaotic line, no identifiable complexes
- Ventricular tachycardia — wide and fast complexes, with or without pulse
- Atrial fibrillation — irregularly irregular rhythm, no defined P waves
- Complete atrioventricular block — complete dissociation between P waves and QRS complexes
- Asystole — isoelectric line, no electrical activity
Repolarization changes:
- ST segment elevation — classic sign of ST-elevation myocardial infarction (STEMI)
- ST depression — subendocardial ischemia or unstable angina
- Prolonged QT interval — risk of torsades de pointes ventricular tachycardia
Vital sign changes:
- Progressive SpO2 drop below 94%
- Sustained hypotension
- Extreme tachycardia or bradycardia
Diagnosis
Continuous cardiac monitoring is not a standalone diagnostic test — it complements clinical assessment and other exams:
12-lead ECG: while the monitor displays 1 to 3 leads in real time, the 12-lead ECG provides a complete view of cardiac electrical activity and is mandatory in any suspected acute coronary syndrome. In the episode, Mr. Gellin's STEMI was identified by 7 mm ST elevation in the anterior leads — what Dr. Robby called tombstones.
Serum troponin: marker of myocardial injury, measured alongside the ECG for risk stratification.
HEART score: risk stratification tool for chest pain combining clinical history, ECG, age, risk factors, and troponin. A score of 0 to 3 indicates low risk — as with Mr. Milton — but does not completely exclude adverse events.
Telemetry: remote cardiac monitoring transmitted to the nursing station by radiofrequency or cable. Allows monitoring of ambulatory patients or those in observation units without confining them to bed.
Emergency Use
Cardiac monitor setup in the emergency room follows a standardized sequence:
- Position electrodes on the patient's clean, dry skin — three electrodes for basic rhythm monitoring, five for full monitoring with precordial lead.
- Connect cables to the monitor and select the lead with the best QRS visualization — usually lead II or V1.
- Configure alarms according to the clinical picture: minimum and maximum heart rate, SpO2 thresholds, blood pressure limits.
- Calibrate the blood pressure cuff and program automatic measurement intervals.
- Connect the pulse oximeter to the finger, earlobe, or forehead.
- Record baseline values and document in the patient chart.
In cardiac arrest situations, the monitor is the first instrument consulted after identifying the absence of a pulse:
- Shockable rhythm (VF or pVT): immediate defibrillation.
- Non-shockable rhythm (asystole or PEA): continuous CPR with search for reversible causes — the Hs and Ts of ACLS.
Post-cardioversion monitoring is also critical — as shown in the episode with patient Quinn after AFib reversal, where the team maintained continuous surveillance for hours to ensure sinus rhythm remained stable.
Prognosis and Complications
The cardiac monitor itself does not cause complications — it is a passive monitoring instrument. However, its improper use has relevant clinical consequences:
- Alarm fatigue: excessive false or low-priority alarms lead teams to ignore critical alerts — a documented problem in ICUs and emergency departments worldwide.
- False sense of security: patients off the monitor may deteriorate without early detection — exactly what happened with Mr. Milton in the hallway.
- Electrical interference: motion artifacts or poorly placed electrodes can simulate serious arrhythmias and trigger unnecessary interventions.
- Skin injury: adhesive electrodes with prolonged use can cause irritation or skin breakdown, especially in neonates and the elderly.
The positive impact of proper monitoring is unquestionable: studies show significant reduction in undetected adverse cardiac events in units with rigorous monitoring protocols and alarm management.

Frequently Asked Questions
Does every ER patient need a cardiac monitor?
No. The indication for continuous cardiac monitoring is clinical, based on risk of deterioration. Low-risk patients — such as those with superficial lacerations, minor sprains, or skin infections without systemic involvement — do not require monitoring. The decision about who to monitor and for how long is a core competency of the emergency physician, as debated in the episode following Mr. Milton's death.
What are tombstones on the ECG?
The term tombstones refers to the pattern of massive, tombstone-shaped ST segment elevation seen in extensive infarctions with total coronary artery occlusion. The shape resembles a cemetery headstone. It is an extremely serious finding associated with a large area of myocardium at risk, and requires immediate activation of the catheterization laboratory for emergency angioplasty.
What is the HEART score?
The HEART score is a risk stratification tool for chest pain patients in the ER. It evaluates five components: History, ECG, Age, Risk factors, and Troponin. Each item scores 0 to 2, totaling up to 10 points. A score of 0 to 3 indicates low risk with a 1% chance of adverse events in 30 days; a score of 7 to 10 indicates high risk with over 50% chance of adverse events.
What is the difference between a cardiac monitor and a Holter?
A hospital cardiac monitor is used in real time at the bedside, with active alarms and a team present to intervene immediately when changes occur. A Holter monitor is a portable ambulatory device worn for 24 to 48 hours — or up to 30 days in long-duration models — recording cardiac rhythm during the patient's daily activities. The Holter is indicated for investigation of intermittent arrhythmias in stable patients — never for emergency monitoring.
Conclusion
The cardiac monitor is an instrument that appears simple at first glance, but whose proper use demands refined clinical judgment. As Episode 3 of The Pitt demonstrates with painful precision, the decision to monitor — or not monitor — a patient can have irreversible consequences.
Explore more about emergency instruments in our Medical Instruments category. Also read about acute myocardial infarction, defibrillator and cardioverter, atrial fibrillation, and cardiac arrest management.
Disclaimer: This content is for educational purposes only and does not substitute professional medical evaluation, diagnosis, or treatment. In case of emergency, call 911 immediately.


