Introduction
The Pitt — Episode 3, atrial fibrillation scene:
"We interrogated his smartwatch. His heart rate has only been up for 92 minutes." — Medical team
"75 of propofol, slow IV push. Sync cardioversion at 200 joules." — Dr. Robby
"Clear. Sinus rhythm. We got him." — Team
This scene from Episode 3 captures synchronized electrical cardioversion with surgical precision: a swift clinical decision, careful sedation, and a millisecond-timed shock that restores the heart to its natural rhythm. In under two minutes, Quinn — the 35-year-old architect in atrial fibrillation — went from a chaotic rhythm to a stable sinus tracing.
Electrical cardioversion is one of the most effective and immediate procedures available in the emergency department. Understanding how it works, when it is indicated, and how it is performed step by step is essential for healthcare professionals, patients, and families who may face this situation.
What is Synchronized Electrical Cardioversion?
Synchronized electrical cardioversion is a procedure in which a controlled electrical current is delivered to the heart in a precisely timed manner — synchronized with the R wave of the electrocardiogram. This synchronization is the most critical element that distinguishes it from conventional defibrillation.

By firing the shock exactly on the R wave, the discharge is prevented from landing during the vulnerable period of the cardiac cycle — specifically the T wave, which represents ventricular repolarization. A shock at that moment could trigger ventricular fibrillation, turning a treatable arrhythmia into a lethal emergency.
The goal is straightforward: interrupt the abnormal electrical circuit sustaining the arrhythmia and allow the sinus node — the heart's natural pacemaker — to resume control of the rhythm. The expected result is conversion to normal sinus rhythm, as achieved with Quinn in the episode.
The procedure is performed using a monitor-defibrillator with SYNC mode activated, ensuring the device recognizes each QRS complex before firing.
Causes and Clinical Context
Synchronized electrical cardioversion is indicated for arrhythmias with a present pulse that cause hemodynamic instability. The main conditions include:
- Unstable atrial fibrillation (AFib): as in the episode, especially when recent onset — under 48 hours — and associated with hypotension, chest pain, or altered consciousness.
- Unstable atrial flutter: generally responds with lower energies, between 50 and 100 joules.
- Refractory supraventricular tachycardia (SVT): when vagal maneuvers and adenosine have failed.
- Ventricular tachycardia with pulse and instability: a high-risk situation requiring immediate intervention.
The clinical trigger for emergency cardioversion is always hemodynamic instability: systolic pressure below 90 mmHg, ischemic chest pain, signs of acute heart failure, or altered level of consciousness. In Quinn's case, the falling blood pressure and heart rate of 147 bpm were the determining factors.
A critical data point in the episode was the 48-hour window: when AFib lasts longer than this period, there is a risk of thrombus formation in the left atrium, and cardioversion may dislodge the clot, causing an ischemic stroke. The smartwatch confirmed 92 minutes of arrhythmia — within the safe window.
Signs and Symptoms
The patient who is a candidate for emergency cardioversion typically presents with:
- Rapid and irregular palpitations of sudden onset
- Hypotension — systolic blood pressure below 90 mmHg
- Dyspnea and progressive shortness of breath
- Chest pain or pressure
- Dizziness, presyncope, or syncope
- Pallor, cold sweating, and cold extremities
- Altered level of consciousness in severe cases
On the cardiac monitor, atrial fibrillation appears as absent defined P waves with an irregularly irregular ventricular response. Atrial flutter shows the classic sawtooth pattern in the inferior leads. Ventricular tachycardia presents wide and regular complexes.
Diagnosis
The decision to cardiovert is based on integrated clinical assessment with the ECG:
12-lead ECG: identifies the exact type of arrhythmia, QRS duration, QT interval, and associated ischemic changes. Mandatory before any elective cardioversion.
Hemodynamic assessment: blood pressure, heart rate, level of consciousness, and peripheral perfusion signs determine urgency. Instability means immediate cardioversion, without waiting for additional tests.
Onset time determination: as demonstrated in the episode, the time of arrhythmia onset is critical. When the patient cannot report it precisely, smartwatch data, family members, or prior medical records can be decisive.
Transesophageal echocardiography (TEE): indicated when AFib has lasted more than 48 hours and cardioversion is elective — rules out left atrial thrombus before the procedure.
The Procedure in the ER
Synchronized electrical cardioversion follows a well-established protocol:
- Confirm indication and obtain verbal consent when possible.
- Set up continuous monitoring: ECG, pulse oximetry, and blood pressure.
- Secure a large-bore peripheral IV access.
- Pre-oxygenate with 100% oxygen mask for 3 minutes.
- Administer fast-acting sedation — in the episode, 75 mg of propofol slow IV push was used. Alternatives include midazolam or etomidate.
- Confirm the patient is sedated and unresponsive to verbal stimulus.
- Activate SYNC mode on the monitor-defibrillator — verify the device is marking QRS complexes with a visual indicator.
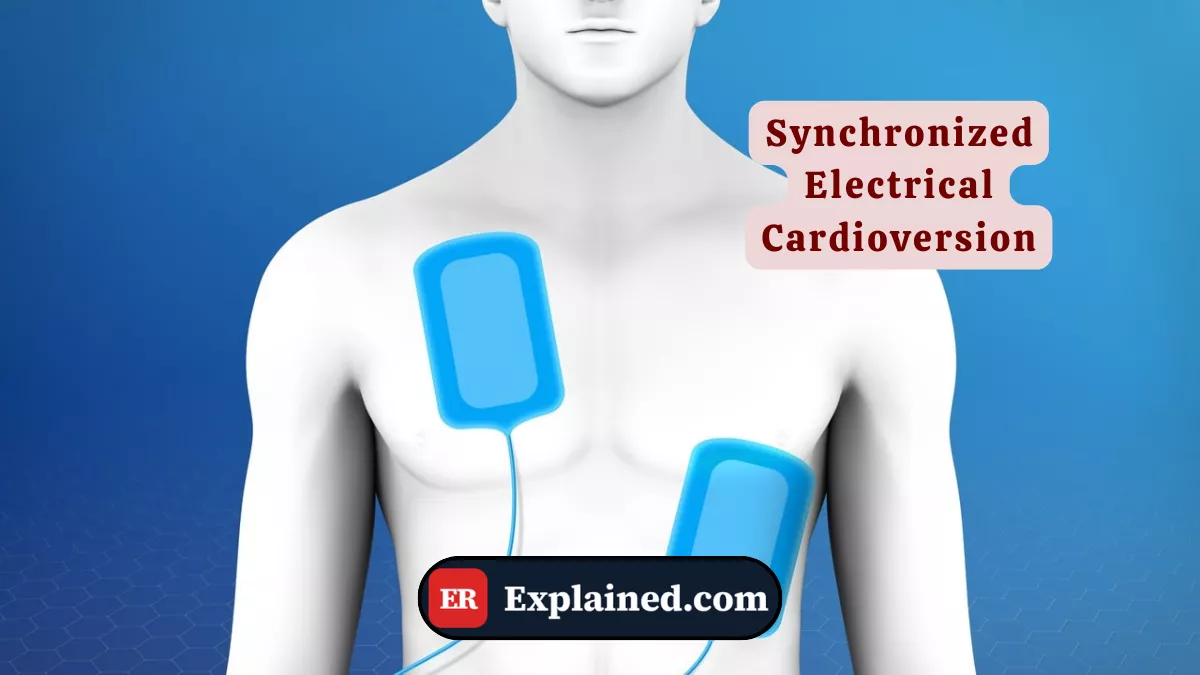
- Position the pads: one below the right clavicle and one at the left midaxillary line.
- Select energy: 120–200 joules for AFib on biphasic devices; 50–100 joules for atrial flutter.
- Announce loudly: "All clear!" — visually confirm no one is touching the patient or stretcher.
- Deliver the shock and immediately observe the monitor to verify the post-shock rhythm.
- If no conversion, reactivate SYNC mode and repeat with escalating energy.
After conversion, monitor the patient for at least 2 to 4 hours. Investigate and treat the underlying cause of the arrhythmia — in the episode, the team referred Quinn to vaping cessation services.
Prognosis and Complications
The success rate of electrical cardioversion for recent-onset AFib exceeds 90% with modern biphasic devices. For atrial flutter, efficacy approaches 95–98%.
The main complications include:
- Systemic embolism or ischemic stroke: primary risk in AFib lasting more than 48 hours without prior anticoagulation or negative TEE for thrombus.
- Post-cardioversion hypotension: related to the sedative agent or transient post-shock myocardial dysfunction.
- Transient arrhythmias: sinus bradycardia, premature beats, or rarely, VF induction from an unsynchronized shock.
- Mild skin burns at the pad sites, especially on dry skin or with body hair.
- Arrhythmia recurrence: patients with structural AFib have high recurrence rates without treatment of the underlying cause.

Frequently Asked Questions
Is electrical cardioversion painful?
In emergency situations, the procedure is always performed under sedation — the patient does not feel pain during the shock. Post-procedure discomfort is minimal and generally limited to mild soreness at the pad sites. The most commonly reported sensation is brief confusion and disorientation in the first few minutes after sedation, which clears quickly.
What is the difference between cardioversion and defibrillation?
Synchronized cardioversion is used for arrhythmias with a present pulse and hemodynamic instability — the shock is timed with the R wave to avoid VF. Defibrillation is used in cardiac arrest with ventricular fibrillation or pulseless ventricular tachycardia — the shock is asynchronous, since there is no organized cardiac cycle to synchronize with.
Do I need anticoagulation before cardioversion?
It depends on how long the AFib has been present. If the arrhythmia lasted less than 48 hours and there is no evidence of thrombus, cardioversion can be safely performed without prior anticoagulation. If it lasted more than 48 hours, anticoagulation for at least 3 weeks beforehand is required — or a TEE must be performed to rule out thrombus — with anticoagulation maintained for 4 weeks after the procedure.
Can AFib return after cardioversion?
Yes. Cardioversion restores the rhythm but does not treat the underlying cause. Patients with structural AFib — associated with hypertension, valve disease, heart failure, or thyroid disease — have high recurrence rates without specific treatment. Outpatient cardiology follow-up is essential to define a sinus rhythm maintenance strategy.
Conclusion
Synchronized electrical cardioversion is one of the most elegant procedures in emergency medicine: a rapid, precise, and highly effective intervention that can transform a potentially fatal arrhythmia into normal sinus rhythm in seconds. As Episode 3 of The Pitt showed, the right decision at the right moment — supported even by data from a smartwatch — can be the difference between stabilization and collapse.
Explore more in our Medical Procedures category. Also read about the defibrillator and cardioverter, atrial fibrillation in the ER, propofol in sedation, and the smartwatch as cardiac monitor.
Disclaimer: This content is for educational purposes only and does not substitute professional medical evaluation, diagnosis, or treatment. In case of emergency, call 911 immediately.

