Introduction
The Pitt — Episode 3, overdose patient scene:
"He's stable and on a vent. Robby wants a few more tests." — Nursing team
"The ventilator is breathing for him. His brain stem is not telling him to breathe." — Dr. Robby
"If we remove the tube, we would keep him on oxygen for comfort." — Dr. Robby
This sequence of scenes from Episode 3 shows the mechanical ventilator in two completely different moments: first as life support for a young man in severe overdose, and then as the only thread still connecting him to existence while the medical team conducts brain death testing.
The mechanical ventilator is one of the most powerful — and ethically complex — pieces of equipment in any ICU or emergency room. Understanding how it works, when it is indicated, and what happens when it is removed is essential for patients, families, and healthcare professionals alike.
What is a Mechanical Ventilator?
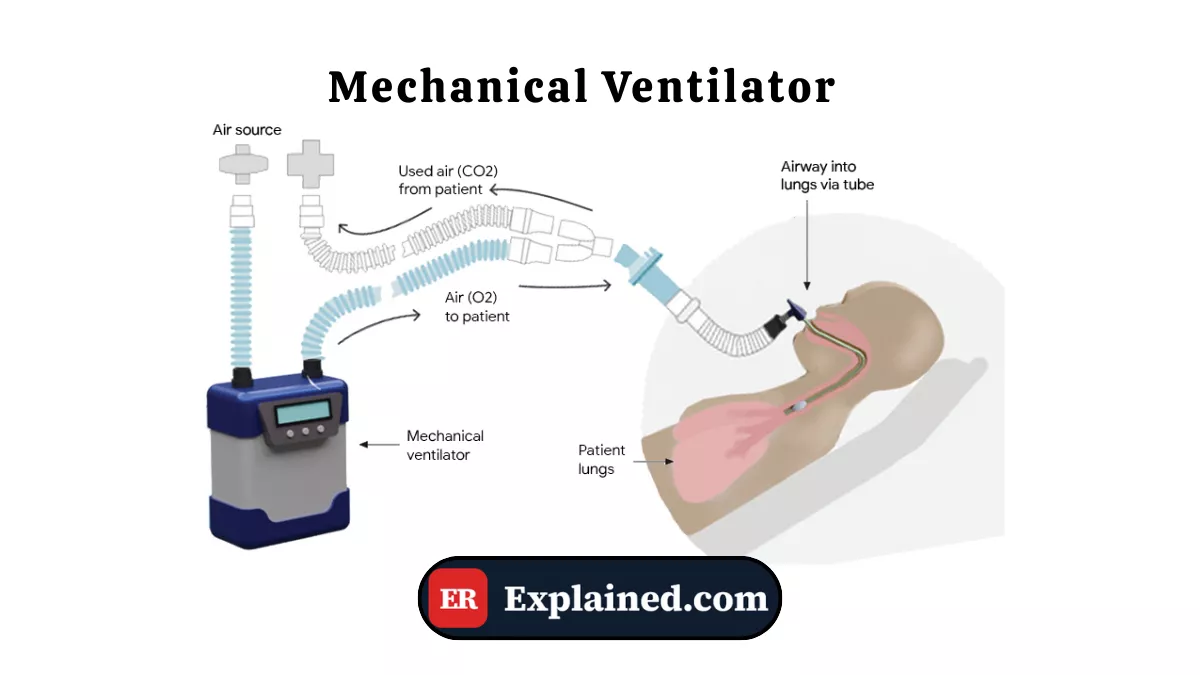
A mechanical ventilator is an electronic device that fully or partially takes over the patient's respiratory work. It rhythmically and precisely inflates the lungs with air — or an air-oxygen mixture — ensuring gas exchange when the patient is unable to breathe spontaneously and effectively.

Operation is based on programmed respiratory cycles:
- Active inspiration: the device generates positive pressure in the airway, pushing air into the lungs.
- Passive expiration: pressure is released and air exits the lungs through elastic recoil.
The main parameters set by the physician include:
- Tidal volume (Vt): the amount of air delivered with each breath, typically 6 to 8 ml/kg of ideal body weight.
- Respiratory rate (RR): number of cycles per minute, typically 12 to 20 breaths/min.
- PEEP (Positive End-Expiratory Pressure): pressure maintained at the end of expiration to prevent alveolar collapse.
- FiO2: fraction of inspired oxygen, from 21% (room air) to 100% (pure oxygen).
- Ventilation mode: controlled, assisted, or pressure support, depending on the patient's level of spontaneous effort.
The ventilator connects to the patient through an endotracheal tube — inserted through the mouth into the trachea — or through a tracheostomy in cases of prolonged use.
Causes and Clinical Context
Mechanical ventilation is indicated whenever the patient cannot maintain adequate ventilation on their own. The main causes that lead to mechanical ventilation include:
- Acute respiratory failure: severe pneumonia, ARDS (Acute Respiratory Distress Syndrome), pulmonary edema.
- Central nervous system depression: opioid, benzodiazepine, or other sedative overdose — exactly the case in the episode, where the young man in fentanyl overdose lost his respiratory drive.
- Cardiac arrest: after resuscitation, patients frequently require ventilatory support.
- Severe traumatic brain injury: with depressed level of consciousness and risk of airway obstruction.
- Major surgery: general anesthesia temporarily suppresses spontaneous breathing.
- Neuromuscular disease: myasthenia gravis, Guillain-Barré syndrome in crisis.
In the episode, patient Nick Bradley was on mechanical ventilation following a fentanyl overdose with cardiac arrest. The ventilator sustained his vital function while the team investigated the extent of brain damage caused by prolonged hypoxia.
Signs and Symptoms
The situations indicating the need for mechanical ventilation present well-defined clinical signs:
Signs of impending respiratory failure:
- Respiratory rate above 35 or below 8 breaths/min
- Use of accessory muscles — neck, intercostals, abdomen
- Suprasternal and subcostal retractions
- Oxygen saturation below 90% despite supplemental O2
- Central cyanosis — blue lips and mucous membranes
- Altered level of consciousness due to hypercapnia or hypoxia
Blood gas criteria for intubation:
- PaO2 below 60 mmHg with FiO2 of 0.5 or more
- PaCO2 above 50 mmHg with pH below 7.25
- Inability to protect the airway
In the episode, the situation was even more critical: the patient had suffered cardiac arrest before arriving at the hospital, with an undetermined period of cerebral hypoxia — making mechanical ventilation a life bridge while the reversibility of neurological damage was assessed.
Diagnosis
The decision to intubate and mechanically ventilate is clinical, but supported by complementary tests:
Arterial blood gas: the most important test for assessing respiratory function. It measures PaO2, PaCO2, pH, bicarbonate, and saturation, guiding the urgency and initial ventilator parameters.
Continuous pulse oximetry: non-invasive monitoring of oxygen saturation. Values below 90% on room air indicate significant hypoxia.
Chest X-ray: identifies pneumonia, pulmonary edema, pneumothorax, or atelectasis that may guide ventilator settings.
Capnography: monitors exhaled CO2 in real time, confirming correct endotracheal tube placement and ventilation efficacy.
Neurological assessment: critical in the episode, where the team used the apnea test and cerebral perfusion scintigraphy to confirm brain death — assessments only possible with the patient already on mechanical ventilation.
Emergency Use
Invasive mechanical ventilation in the emergency setting follows well-defined steps:
Orotracheal intubation
- Pre-oxygenation with 100% oxygen mask for 3 to 5 minutes.
- Administration of sedation and neuromuscular blockade — in Hank's episode scene, ketamine 100 mg and succinylcholine 120 mg IV were used.
- Direct laryngoscopy or videolaryngoscopy to visualize the vocal cords.
- Insertion of the endotracheal tube through the glottis, confirmed by capnography and auscultation.
- Tube fixation and connection to the mechanical ventilator.
Recommended initial settings
- Mode: volume-controlled ventilation (VCV) or pressure-controlled (PCV) based on the clinical picture.
- Tidal volume: 6 ml/kg of predicted body weight — lung-protective strategy to prevent ventilation-induced lung injury.
- Initial PEEP: 5 cmH2O, adjusted based on oxygenation.
- Initial FiO2: 100%, progressively reduced to maintain SpO2 between 94% and 98%.
- Respiratory rate: 12 to 16 breaths/min, adjusted by blood gas results.
Ventilator weaning
Weaning — the process of progressively reducing support until extubation — is initiated once the cause that led to ventilation has been reversed. Criteria include hemodynamic stability, improved gas exchange, preserved level of consciousness, and ability to protect the airway.
In Nick Bradley's case, weaning was never a possibility: the apnea test confirmed absence of spontaneous respiratory drive, and the scintigraphy demonstrated absence of cerebral blood flow — diagnostic criteria for brain death.
Prognosis and Complications
Mechanical ventilation saves lives but is not without risk. The main complications include:
- Ventilator-associated pneumonia (VAP): pulmonary infection caused by microorganisms colonizing the endotracheal tube. It is the most frequent infectious complication in the ICU.
- Ventilator-induced lung injury (VILI): alveolar damage caused by excessive volumes or pressures — prevented by lung-protective ventilation strategies.
- Pneumothorax from barotrauma: alveolar rupture from excessive pressure.
- Muscle weakness from disuse: diaphragm and respiratory muscle atrophy with prolonged ventilation.
- Ventilator dependence: difficulty weaning in patients with severe lung disease or neurological impairment.
Prognosis depends fundamentally on the underlying disease. In overdoses with rapid treatment and no prolonged hypoxia, full recovery is possible. In the episode, the time of cardiac arrest before treatment was the determining factor in the tragic outcome.

Frequently Asked Questions
Is a patient on a ventilator always unconscious?
Not necessarily. Many patients on mechanical ventilation are awake and conscious, especially during non-invasive ventilation or the weaning process. During invasive ventilation, patients generally receive sedation to tolerate the endotracheal tube — but the level of sedation varies by clinical picture. In the episode, the overdose patient was sedated and neurologically unresponsive, which was a sign of severity, not a consequence of sedation.
How long can a patient remain on a ventilator?
There is no fixed limit. Patients with severe chronic diseases may require ventilation for weeks, months, or permanently. In general, ventilation for more than 7 to 14 days calls for evaluation for tracheostomy, which is more comfortable and facilitates weaning. The goal is always early weaning as soon as the clinical condition allows.
What is the apnea test?
The apnea test is one of the criteria for diagnosing brain death. The ventilator is set to deliver no breaths — the patient receives oxygen but no active ventilation. Blood CO2 is monitored for 10 minutes: if CO2 rises above 60 mmHg without any spontaneous respiratory effort, the brainstem is not functioning. In the episode, Nick's CO2 reached 82 mmHg with no spontaneous breathing — confirming brain death.
Is removing the ventilator the same as killing the patient?
No, from a medical and ethical standpoint. When brain death is confirmed through rigorous criteria — as in the episode — the patient is already dead, and the ventilator merely sustains residual organic functions through mechanical pressure. Withdrawal of ventilatory support in confirmed brain death is an act of respect for the patient's dignity and is supported by medical protocols and legal frameworks in both Brazil and the United States.
Conclusion
The mechanical ventilator is simultaneously an instrument of salvation and a mirror of the most difficult questions in modern medicine. As shown in Episode 3 of The Pitt, it can be both the bridge to recovery for a young man in overdose and the thread that sustains existence while a family finds the strength to accept the unacceptable.
Explore more about emergency medicine instruments in our Medical Instruments category. Also read about orotracheal intubation, brain death, ketamine in emergency sedation, and endotracheal tube.
Disclaimer: This content is for educational purposes only and does not substitute professional medical evaluation, diagnosis, or treatment. In case of emergency, call 911 immediately.


