The Sympathetic Storm
"Her medical history says she had a malignant pheochromocytoma removed five years ago. That explains the bizarre hypertensive crisis she just had." — Emergency Room
In medicine, certain diseases are known as "great mimickers" because their symptoms look like dozens of other, more common conditions. One of the rarest and most dangerous of these mimickers is the Pheochromocytoma.
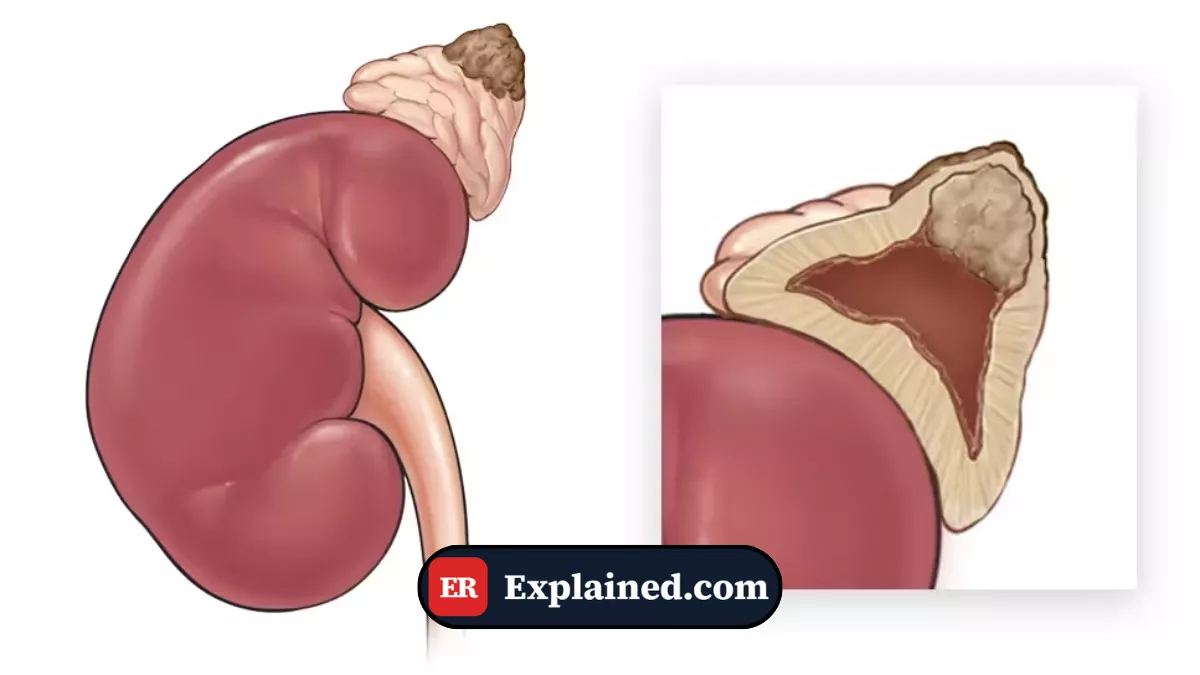
A pheochromocytoma is a rare tumor that grows in the adrenal glands (the small glands that sit on top of each kidney). What makes this tumor so lethal is not its size, but what it produces.
The adrenal glands are responsible for producing the body's adrenaline (epinephrine) for the "fight or flight" response. A pheochromocytoma is essentially a runaway factory that pumps massive, random amounts of adrenaline and noradrenaline directly into the bloodstream.

The Attacks: A System Overload
Patients with this tumor frequently live normal lives until the tumor decides to "fire." Without warning, the body is flooded with adrenaline levels 10 to 50 times higher than normal.

This causes a classic triad of symptoms during the "attacks" (paroxysms):
- Pounding Headaches: So severe they are frequently misdiagnosed as migraines or aneurysms.
- Palpitations and Tachycardia: The heart beats so hard and fast the patient feels like they are having a heart attack.
- Profuse Sweating: The patient becomes drenched in sweat, even in a cold room.
Behind these visible symptoms, a massive Hypertensive Crisis occurs. The patient's blood pressure can shoot from a normal 120/80 to a lethal 250/140 in minutes. If unchecked, this pressure can blow blood vessels in the brain (causing a stroke) or tear the aorta.
The Danger in the Emergency Room
The greatest danger of a pheochromocytoma is that the wrong treatment in the ER will kill the patient instantly.
If a patient arrives with a blood pressure of 240/130 and the doctor does not know about the tumor, the natural instinct is to give a "beta-blocker" (like Metoprolol or Labetalol) to bring the pressure and heart rate down.
In a patient with a pheochromocytoma, giving a beta-blocker alone is a death sentence. Adrenaline acts on two receptors in the body: Alpha (which squeezes blood vessels) and Beta (which relaxes vessels and speeds up the heart). If you block only the Beta receptors, all that massive adrenaline floods the Alpha receptors. The blood vessels will clamp down so hard that the blood pressure will spike even higher, causing immediate cardiac arrest.
The Correct Treatment and Cure
If the doctor suspects the tumor, medical management must follow a strict order:
- Alpha Blockade FIRST: The patient must be given alpha-blockers (like Phentolamine or Phenoxybenzamine) to force the blood vessels open and drop the blood pressure.
- Beta Blockade SECOND: Only after the alpha blockade is fully established (frequently days later) can doctors add beta-blockers to control the heart rate.
The definitive cure is purely surgical: removing the entire adrenal gland. The surgery itself is incredibly dangerous, as the mere touch of the surgeon's scalpel on the tumor can cause it to dump one last massive dose of adrenaline. Highly specialized anesthesiologists are required to manage the patient's blood pressure second-by-second during the operation.
Frequently Asked Questions (FAQ)
Why are most pheochromocytomas discovered by accident?
Because the symptoms (headache, sweating, anxiety) look exactly like severe panic attacks or anxiety disorders. Many patients spend years being treated by psychiatrists before someone orders a CT scan of the abdomen for another reason (like a kidney stone) and accidentally finds the tumor (an "incidentaloma").
Is the tumor cancerous?
In most cases (about 90%), the pheochromocytoma is benign (it does not spread to other organs). However, the word "benign" here is misleading, as the adrenaline it produces is frequently fatal. About 10% are malignant and spread to the bones or liver.
How is the diagnosis confirmed?
The definitive diagnosis is made by measuring the waste products of adrenaline (called metanephrines) in the patient's urine or blood. Patients must collect all their urine in a jug for 24 hours to catch the levels during an attack.
Conclusion
Pheochromocytoma is a rare disease that demands perfect pharmacological knowledge. It is the ultimate reminder in medicine that treating a number on the monitor (like high blood pressure) without understanding the underlying cause can be disastrous. For the patient, the removal of the tumor frequently feels like a miracle, instantly curing years of terrifying "panic attacks" and untreatable high blood pressure.
This content is for educational and informational purposes only. It does not replace professional medical advice, diagnosis, or treatment. In case of a medical emergency, call 911/EMS immediately or go to the nearest emergency room.
References: [1] National Cancer Institute: Pheochromocytoma [2] StatPearls: Pheochromocytoma [3] UpToDate: Clinical presentation and diagnosis of pheochromocytoma [4] EMCrit: Hypertensive Emergencies

