The Lung That Suffocates Itself
"Joyce's oxygen saturation is dropping. She has a new infiltrate on her chest x-ray. It's Acute Chest Syndrome. Start the exchange transfusion and antibiotics immediately." — Emergency Room
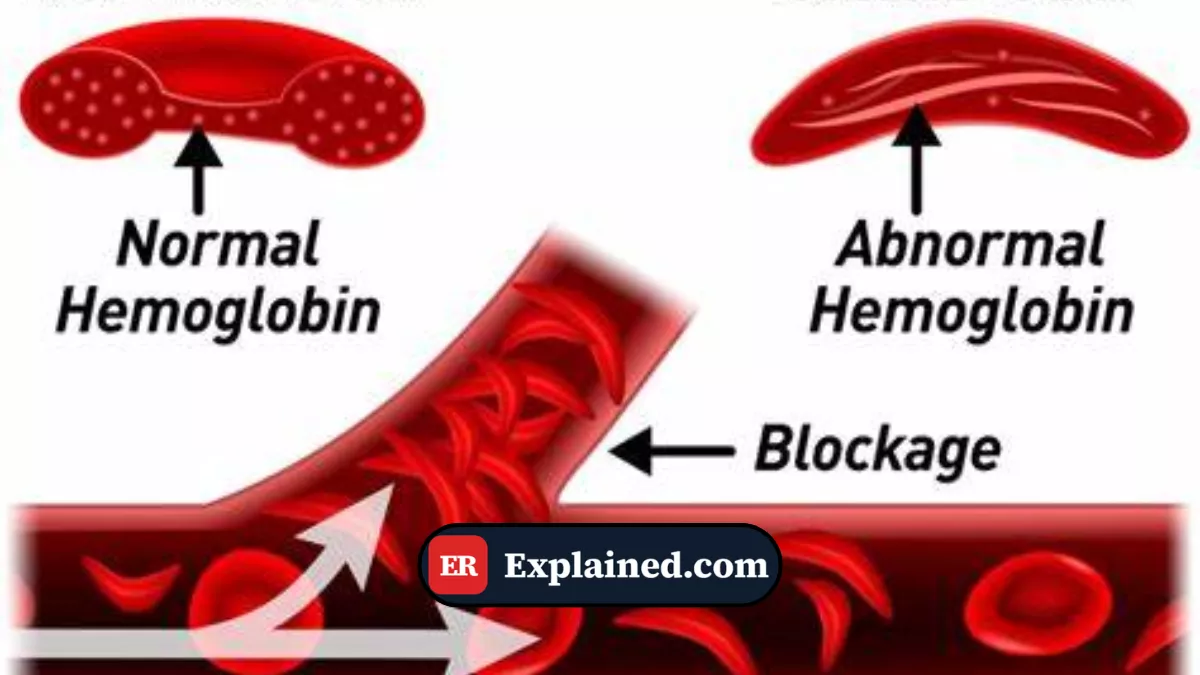
Sickle Cell Disease is a devastating genetic disorder that alters the shape of red blood cells. Instead of being flexible, round discs that glide easily through blood vessels, they become rigid and shaped like a sickle (crescent moon).
The most common complication is the "pain crisis," where these cells clump together and block blood flow to the bones and joints. However, the most feared complication and the leading cause of death in sickle cell patients is Acute Chest Syndrome (ACS).
ACS occurs when these sickle-shaped cells begin to block the tiny blood vessels inside the lungs themselves, triggering a lethal cycle of asphyxiation and inflammation.

The Vicious Cycle of ACS
Acute Chest Syndrome rarely starts out of nowhere. It frequently develops while the patient is already in the hospital being treated for a pain crisis. The trigger can be a mild lung infection, a broken bone releasing fat into the blood (fat embolism), or simply the patient taking shallow breaths due to rib pain.

Once triggered, ACS feeds on itself:
- Local Hypoxia: A small area of the lung is deprived of oxygen (due to infection or shallow breathing).
- Sickling: Sickle red blood cells are highly sensitive to low oxygen. When they hit this low-oxygen area, they instantly snap into the sickle shape.
- Blockage: The sickled cells clog the pulmonary blood vessels (pulmonary infarction).
- More Hypoxia: The blockage causes even less oxygen in the lung, which causes more cells to sickle, clogging more vessels.
Within hours, a patient who was merely having leg pain can be fighting for their life on a mechanical ventilator, with their lungs completely white (infiltrates) on an x-ray.
Diagnosis and Warning Signs
Diagnosing ACS in the emergency room requires three things:
- A patient with a known history of Sickle Cell Disease.
- A chest x-ray showing a "new infiltrate" (a white patch on the lung that was not there before).
- Respiratory symptoms: Fever, cough, chest pain, rapid breathing, or dropping oxygen levels.
The challenge is that ACS looks exactly like severe pneumonia on an x-ray, and frequently the two conditions co-exist (the infection causes the sickling).
Aggressive ICU Treatment
Treating ACS cannot wait. It requires immediate intervention to break the vicious cycle:
- Oxygen and Respiratory Support: High-flow oxygen, frequently using BiPAP or intubation, to force oxygen into the lungs and stop the sickling process.
- Exchange Transfusion: The definitive treatment. A machine removes the patient's sickled blood and replaces it with healthy donor blood. The goal is to drop the percentage of sickle cells in the body to below 30%.
- Broad-Spectrum Antibiotics: Because it is impossible to instantly distinguish ACS from pneumonia, doctors always assume there is an atypical bacterial infection. They use a Cephalosporin (like Ceftriaxone) paired with a Macrolide (like Azithromycin).
- Careful Pain Control: The patient needs Morphine for the excruciating pain, but doctors must be extremely careful. If they give too much morphine, the patient will breathe slower, worsening the lack of oxygen in the lungs.
Frequently Asked Questions (FAQ)
Why is the incentive spirometer so important?
Patients in a pain crisis are frequently handed a small plastic tube with a ball inside (incentive spirometer) and told to take deep breaths every hour. This forces the air sacs at the bottom of the lungs open, preventing lung collapse (atelectasis) which is the primary trigger for Acute Chest Syndrome.
Can ACS happen in children?
Yes, it is extremely common in children with sickle cell disease. However, ACS in children is frequently triggered by viral infections (like RSV or the flu) and tends to be less lethal than in adults, where it is frequently caused by fat embolisms from dying bones.
What is the difference between a normal pain crisis and ACS?
A normal vaso-occlusive crisis (pain crisis) causes extreme pain in the bones (arms, legs, back), but the lungs are clear and oxygen is normal. ACS specifically involves the lungs, causing shortness of breath, dropping oxygen, and spots on the x-ray. A pain crisis can turn into ACS in a matter of hours.
Conclusion
Acute Chest Syndrome is the most critical emergency in Sickle Cell Disease management. It requires emergency doctors to look past the pain control and aggressively monitor the patient's lungs. Rapid exchange transfusion and respiratory support are the only ways to stop the lethal cascade of sickled cells suffocating the lung from the inside out.
This content is for educational and informational purposes only. It does not replace professional medical advice, diagnosis, or treatment. In case of a medical emergency, call 911/EMS immediately or go to the nearest emergency room.
References: [1] American Society of Hematology (ASH): Sickle Cell Guidelines [2] StatPearls: Acute Chest Syndrome [3] Centers for Disease Control and Prevention (CDC): Sickle Cell Disease [4] UpToDate: Acute chest syndrome in adults with sickle cell disease

