The Never-Ending Fight
"He's been down for 40 minutes. We've pushed 5 rounds of epi. Still in asystole. I think it's time to call it." — Emergency Room
Most people know Cardiopulmonary Resuscitation (CPR) through movies: a few minutes of chest compressions, a shock from a defibrillator, and the patient coughs and wakes up.
In the brutal reality of emergency medicine, cardiac arrest is frequently a prolonged, exhausting battle. And sometimes, it becomes what doctors call Refractory Cardiac Arrest.
This occurs when the patient receives high-quality CPR, multiple doses of epinephrine, and multiple shocks, but the heart stubbornly refuses to restart (failure to achieve Return of Spontaneous Circulation - ROSC).
The ACLS Algorithm and Its Limits
The treatment of cardiac arrest follows the Advanced Cardiovascular Life Support (ACLS) protocol. The team runs like a well-oiled machine:

- Uninterrupted Compressions: 100 to 120 per minute, switching compressors every 2 minutes to prevent fatigue.
- Airway Control: Intubation to ensure oxygen reaches the lungs.
- Medications: Epinephrine (Adrenaline) injected every 3 to 5 minutes to try and force blood vessels to clamp down and push blood to the heart.
- Defibrillation: Electrical shocks if the rhythm is "shockable" (Ventricular Fibrillation or pulseless Ventricular Tachycardia).
But what if you do this for 20, 30, or 40 minutes and the monitor still shows a flatline (asystole)? This is where the standard algorithm ends and the hard decisions begin.
Hunting for the "H's and T's"
During a refractory arrest, the lead doctor must physically step back from the bed, close their eyes for a second, and think deeply. They are hunting for reversible causes, known mnemonically as the H's and T's:
- H's: Hypovolemia (blood loss), Hypoxia (lack of oxygen), Hydrogen ion (severe acidosis), Hypo/Hyperkalemia (abnormal potassium), Hypothermia.
- T's: Tension pneumothorax, Tamponade (cardiac), Toxins (overdose), Thrombosis pulmonary (embolism), Thrombosis coronary (massive heart attack).
If the doctor can identify and fix one of these causes (e.g., draining blood from the pericardium or giving calcium for hyperkalemia), the heart will frequently restart almost immediately.
The Exhaustion Factor and the LUCAS Device
Manual CPR exhausts even the fittest first responders in minutes. Weak compressions do not save lives.
In prolonged arrests, hospitals frequently use mechanical CPR devices, such as the LUCAS. This machine wraps around the patient's chest and delivers perfect, deep, uninterrupted compressions, freeing up the human team to focus on finding the cause of the arrest and preparing medications.
When to "Call It"
The hardest decision in medicine is deciding when to stop trying. There is no universal magic time limit, but doctors consider several factors:
- Downtime: How long was the patient without CPR before the ambulance arrived? If it was 15 minutes, the brain is already dead.
- The Rhythm: Continuous asystole (flatline) has a near-zero survival rate.
- ETCO2 Levels: Capnography measures exhaled carbon dioxide. If the level drops below 10 mm Hg after 20 minutes of CPR, it proves the body's cells are no longer producing energy. It is a definitive sign of cellular death.
- Age and Comorbidities: A 20-year-old with hypothermia might get CPR for hours. A 90-year-old with terminal cancer will have resuscitation halted much sooner.
When the lead doctor finally says "Time of death...", the room suddenly goes quiet. The machines are turned off, and the team must immediately compose themselves to see the next patient.

Frequently Asked Questions (FAQ)
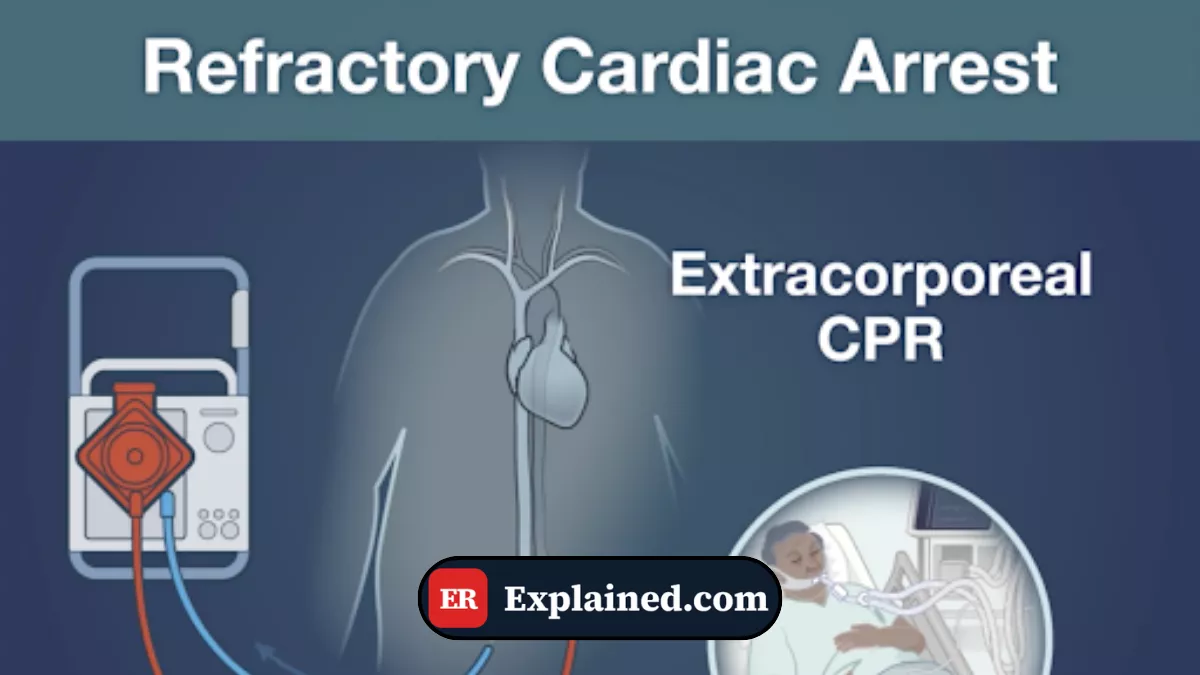
What is ECMO-CPR (ECPR)?
It is the absolute cutting edge of resuscitation. In top-tier hospitals, if a young patient has a refractory cardiac arrest, doctors can hook them up to an ECMO (Extracorporeal Membrane Oxygenation) machine while CPR is ongoing. The machine pumps and oxygenates the blood outside the body, essentially replacing the dead heart and lungs, giving doctors hours or days to fix the original problem.
Does epinephrine (adrenaline) actually work?
It is a topic of intense medical debate. Epinephrine definitely helps restart the heart (ROSC). However, recent studies show it clamps down blood vessels so hard that it can decrease blood flow to the brain. Therefore, patients who get too much epinephrine might get their hearts restarted, but frequently suffer severe brain damage.
Why not shock a flatline (asystole)?
A defibrillator does not "jump-start" the heart. It actually stops the heart for a fraction of a second, hoping the heart's natural pacemaker will take over in a normal rhythm. If the heart is already flatlining (no electrical activity), shocking it will do absolutely nothing. The only hope is CPR and epinephrine.
Conclusion
Refractory cardiac arrest is the ultimate test of a medical team's endurance. It is a brutal balance between aggressive hope (hunting for reversible causes, using compression machines) and the humble recognition of the limits of medical science.
Knowing how to run a perfect "code" is a technical skill; knowing when to stop torturing a lifeless body and allow for a dignified death is the true art of emergency medicine.
This content is for educational and informational purposes only. It does not replace professional medical advice, diagnosis, or treatment. In case of a medical emergency, call 911/EMS immediately or go to the nearest emergency room.
References: [1] American Heart Association (AHA): CPR & ECC Guidelines [2] StatPearls: Advanced Cardiac Life Support (ACLS) [3] EMCrit: ECMO-CPR (ECPR) [4] UpToDate: Advanced cardiac life support (ACLS) in adults